
You're doing everything required to run a compliant LTSS program. Einra is how you start proving it's working.
LTSS leaders are navigating HCBS compliance, state partner relationships, and medical spend targets at the same time. But without a signal from what's happening in members' homes between visits, your care team finds out too late to intervene — and the claims tell you afterward.
Einra routes what paid caregivers observe — in real time — to your MCO coordinator and home health agency, with evidence-based interventions ready. Earlier intervention. Fewer admissions. Clinical outcomes your state partner can see, medical spend your boss can measure, and VBP performance that strengthens your case at reprocurement.
By the time the care coordinator hears, it can already be a crisis.
Every time we reduce a fall, we increase the chance they can age at home.
The blind spot between visits is where cost is created.
Avoidable hospitalizations and facility transitions rarely start as emergencies. They start as in-home deterioration that no one routes to the care team in time. LTSS is a disproportionate share of Medicaid spend, so the most expensive outcomes begin as signals that never reach the care team.
What aides notice — changes in mobility, difficulty with meals, pain, shifts in mood — can reliably predict an ER visit within 7 days.
A study of 301 older adults living at home confirmed it. The aides logged observations on their phones. The predictions held up with strong statistical accuracy.
Veyron et al., 2019 · peer-reviewed · community-dwelling adults age 75+
Dorothy's paid caregiver witnessed her fall twice. Because there was no injury, nothing was reported — and the health plan was blind to it. No way to carry those signs to anyone who could act. The third fall sent her to the hospital.
The smoke detector was going off the whole time. It just wasn't connected to anything.
"I can't put out the fire if nobody tells me there's smoke."
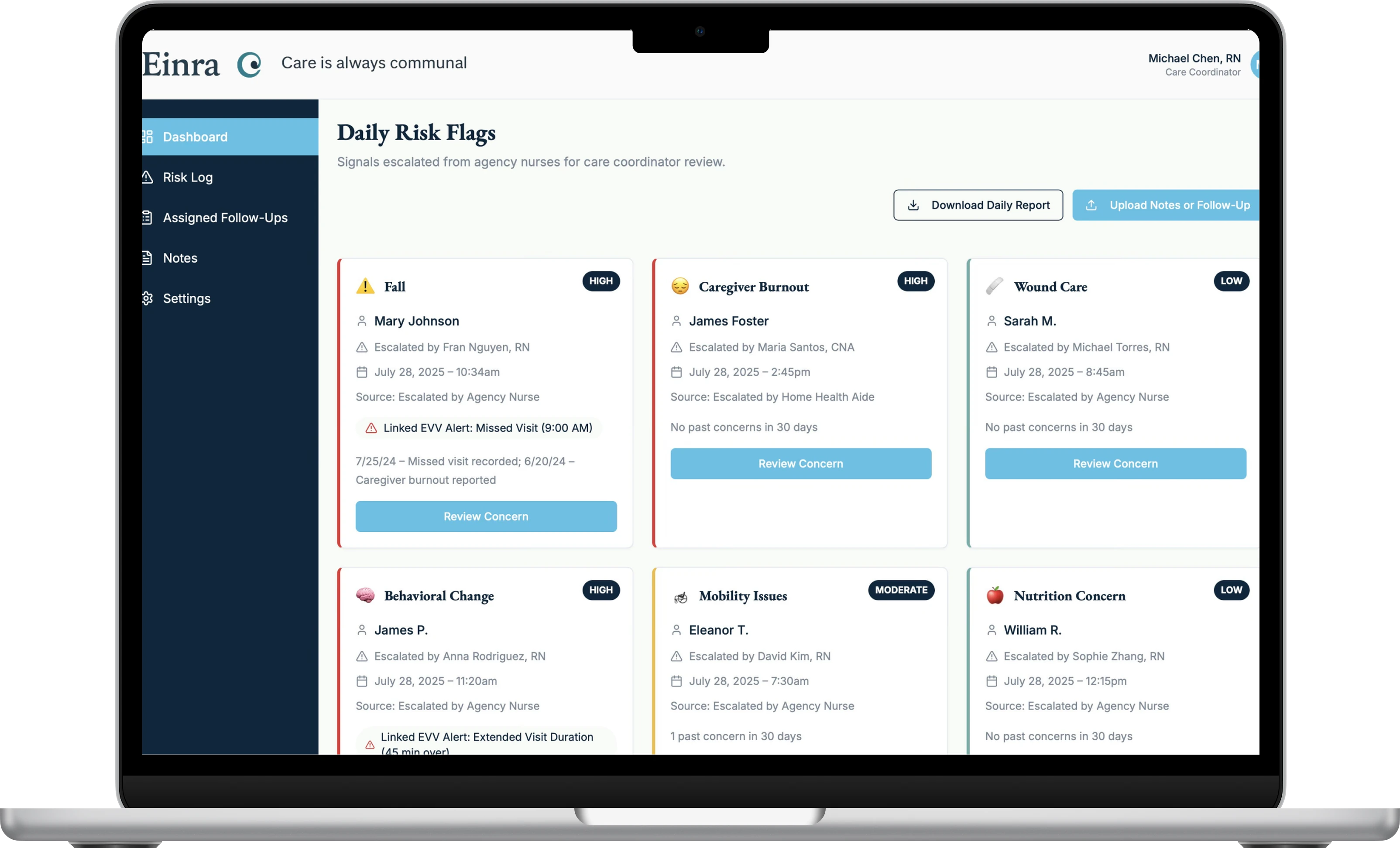
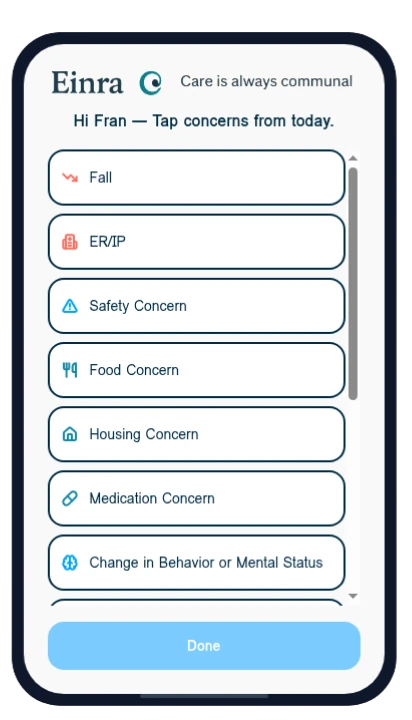
The smoke detector for home-based care. Aides catch risks before they become a crisis. Those risks are routed to your care team in time to act.
Eight clinically validated risk signals — the in-home changes that reliably predict a crisis. Signals, not noise.
Einra reads each one for early risk and routes it, in real time, to the right coordinator. In real time, not in hindsight.
The care team intervenes before the ER visit, before the admission, before the transition. Ahead of the crisis, not after it.
Service Coordinators and Care Coordinators confirm the in-home signal is real, and that they can act on it.
"Claims don't tell us soon enough. Aides see it first."
"I can think of three members this year where, if I'd known sooner, we could have prevented an ER visit."
"I feel like I'm flying blind most of the time — I don't know the full picture of what's happening in the home."
"The frontline aides see things before we do, but their observations rarely make it back to us in time."
"If we could catch the little fires before they turn into a brush fire, that's everything."
The people closest to the member already see risk first. Einra is the channel that finally carries what they see to the care team.
Proven by hand. Built to scale.
Before Einra, the founder — a Medicaid LTSS operator and RN inside a large MCO — built and ran the manual version of this model for roughly 500 high-risk members. What that hands-on program delivered:
We built Einra to scale that model.
We validated the hardest question first: will aides actually use the tool, and does the care team find it valuable?
A 6-week study with agency nurses, paid caregivers, and MCO care coordinators, run on realistic but fictional member scenarios. No member data was collected or used — a test of the workflow, not a clinical trial.
"Perfect. Simple. Easy. No need for improvement."
Paid caregiver · workflow validation participant"I think this [Einra] is the way to prevent hospitalizations."
MCO care coordinator · workflow validation studyThe rules — and the economics — just changed.
MCOs now have to prove — publicly — that what they pay for HCBS is adequate. Demonstrable outcomes are becoming table stakes.
The same MCO will have to own both Medicare and Medicaid for dual-eligible members — putting the full cost of care under one roof.
With rates fixed, every avoidable admission comes straight off the margin — so managing avoidable spend matters more than ever.
"I love it already, and I love the simplicity and depth of the use case."
"VBP isn't VBP if it isn't agile. What you're building creates the flexibility we're missing."
Your staff will use what brings them value.
This is an MCO tool, and adoption is the whole game. Care and service coordinators don't need zero friction — they need a signal worth crossing the street for. Einra surfaces risk early, before it becomes a crisis, and gives the care team something they can act on the moment they see it.
"You walk away knowing you helped someone stay in their home."
Prove it in one LTSS product with a 90-day pilot.
A low-lift overlay. No replacements, no EHR integration. Active signal flow with a readout at Day 45 and a go or no-go at Day 90. If the pilot ends, your operations are fully restored.